①異物である手術材料を最小限にして、成長を期待して自己組織を積極的に使った修復
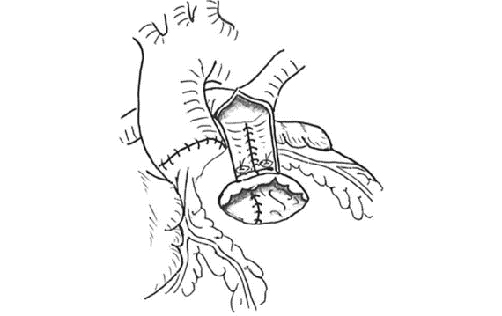
“Repair of persistent truncus arteriosus without a conduit: sleeve resection of the pulmonary trunk from the aorta and direct right ventricle-pulmonary artery anastomosis”
Establishing a new continuity between the right ventricle and the pulmonary artery is the mainstay of repair for persistent truncus arteriosus. We used the Tran Viet-Neveux technique without a Lecomte maneuver to construct the connection without a conduit. Here, we retrospectively review the mid-term surgical results to examine the effectiveness of this approach.
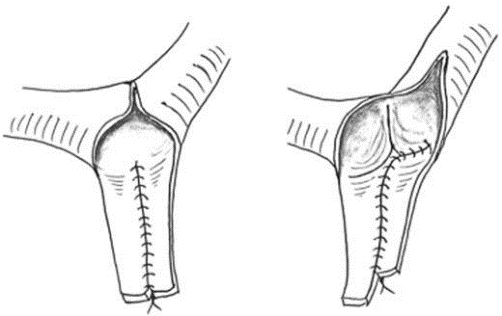
A cylindrical segment incorporating both pulmonary artery branches was sleeve-resected from the truncal artery. The cylindrical segment was cut in the middle and two truncal arterial flaps were combined to form the posterior floor of the new pulmonary arterial trunk. The edge of the floor was attached directly to the superior margin of an oblique incision made in the left-anterior wall of the right ventricle. A polytetrafluoroethylene monocusp was attached to the lower half margin of the right ventricular incision. A large glutaraldehyde-treated pericardial patch was used to form the anterior hood of the new right ventricular outflow tract. Both great arteries were located in a normal spiral configuration.
Ten babies (range: 3 days to 9 months of age) underwent this procedure. The Collett-Edwards classification of persistent truncus arteriosus was type I in five cases and type II in five others. There was one hospital death due to severe respiratory distress. During follow-up (36-60 months, median 54 months), only one re-operation was required to enlarge a left branch pulmonary artery stenosis. Follow-up echocardiography showed pulmonary regurgitation (mild two, moderate seven, and severe one) and mild flow acceleration in the left pulmonary artery branch and right ventricle-pulmonary artery connection in one case.
This simple modification for surgical correction of persistent truncus arteriosus may be an effective alternative that overcomes conduit-related problems.
②自然な弁機能を維持した手術
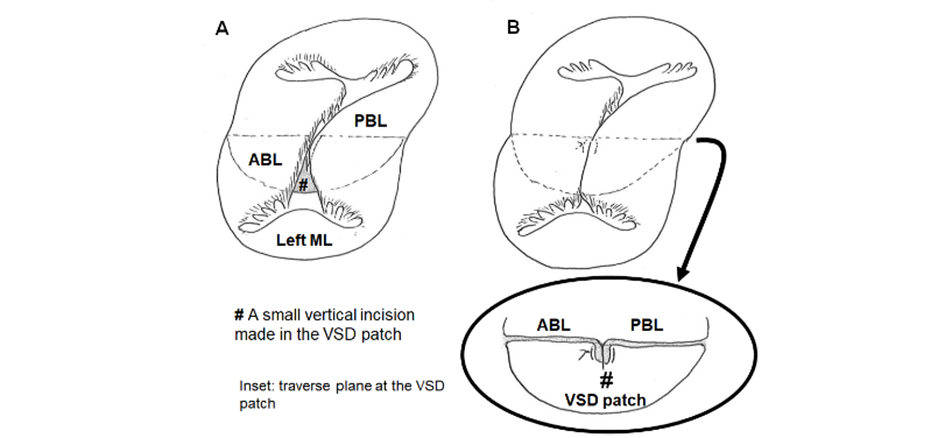
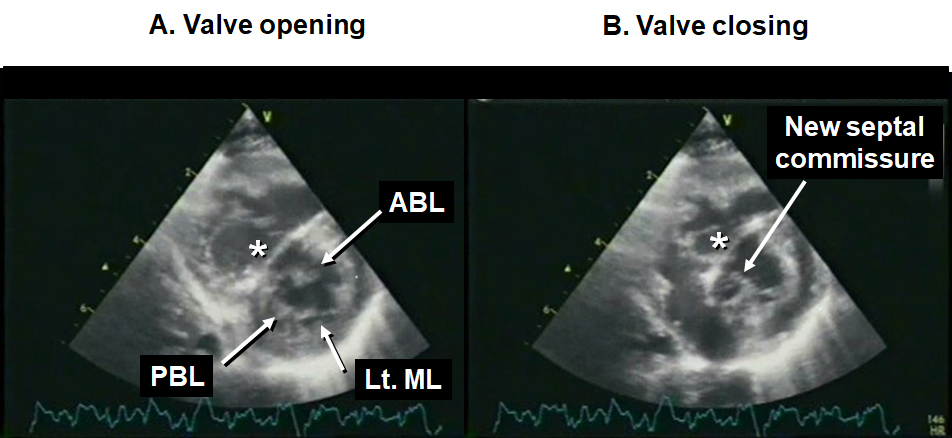
“いわゆる“cleft”を中隔交連として温存した 完全型房室中隔欠損症two-patch修復術”
完全型房室中隔欠損症修復術における左側房室弁修復の良否は術後の予後を左右する重要な要素です。従来 のtwo-patch法では、水平な心室中隔欠損閉鎖パッチ (VSDパッチ)の上端で左側前後共通弁尖間の生理的な接合を 消失させ“cleft”として全閉鎖し左側房室弁を二尖化することに重点が置かれています。われわれはこの前後共通弁尖 間の接合を左側中隔交連として再構築し生理的な弁構造を維持することで“cleft”全閉鎖に頼らない術式を行っています。その早期~中期成績を検討しました。 方法:対象は本術式を施行した自験連続26例.男女比 = 15/11,手術時年齢は平均 7 カ月(1~39),Down症19/26, 中等度以上の肺高血圧症22/26.合併心内病変は筋性部心室中隔欠損 4,二次孔心房中隔欠損または卵円孔開存 18,Fallot四徴症 2.先行手術は肺動脈バンディング 2,Blalock-Taussig短絡 2,大動脈縮窄解除 1.共通弁尖形態は Rastelli A型 7,B型 2,C型17.左側壁側尖の低形成 6,共通房室弁閉鎖不全 5.手術は心室中隔欠損孔をパッチ閉 鎖後に同パッチ上縁に作成した垂直スリットに前後共通弁尖の交連を挿入固定し,一次孔心房中隔欠損をグルタルアルデヒド処理自己心膜パッチで閉鎖.いわゆる “cleft”閉鎖はなし 8,パッチ側交連部のみ13,全長閉鎖 5. 交連部縫縮等の追加弁形成手技 10.同時手術は肺動脈形成 2,右心室流出路形成 2,筋性部心室中隔欠損閉鎖 2. 成績:手術死亡 0,外科的房室ブロック 0.再手術は左側房室弁形成 2(術後 1,12日目),筋性部心室中隔欠損閉鎖 1 (術後 3 日目).退院後平均36.2カ月(14~39カ月)での死亡 0,中等度以上の左側房室弁閉鎖不全 5 (4 例は無症状で 投薬を必要とせず,1 例はアンジオテンシン変換酵素阻害剤とアドレナリン受容体遮断剤投与下に経過観察中). 結論:修復後の前後共通弁尖の接合を“cleft”全閉鎖に頼らない本術式の早期~中期成績は良好であり,長期成績からの再評価が待たれます。特に “cleft”全閉鎖が不可能な左側房室弁口狭小例や左側壁側尖の低形成例に対するtwopatch法の変法として簡単に付加できる有効な選択肢の一つであることが示唆されました。